
Last summer an Italian unicorn founder from the Silicon Valley who built one of the most credible patient data companies in the US pinged us saying: “There’s an Italian team in Berlin building something I wish I built myself.”
A few days after we get connected and we started to get to know the founders. The first thing Mattia said to me was that he was building “the Bloomberg terminal for pharma commercial teams.” I had just moved back to Italy after ten years in London so every time I hear “Bloomberg terminal”, I immediately think about the thing you open before your coffee, the thing whose absence would genuinely break your day. So when someone reaches for that comparison, I hear: this is infrastructure people will not be able to work without.
In this post I want to share why we invested in mama health, how we got comfortable with the hardest parts of the thesis, and what we’ve learned watching the team over the last few months.
Best,
Virgi
The most expensive blind spot in the world
Here is something about pharma that I think most people outside it don’t fully appreciate. You spend 15 years building a drug. You navigate trials, regulators, approval processes. You burn through hundreds of millions (the average cost to commercially launch a new drug is around $500m). There are roughly 78 new drug launches globally every year. And then, after all of that, you walk out the door and face the market: 40% of those launches don’t meet expectations.
This happens because the team launching didn’t deeply understand who the patient really was, what their life looked like, what was keeping them from seeking care, why they stopped a treatment that was working, what emotional barrier sat between awareness and action. And that’s because this market is structurally opaque. The patient’s journey happens in fragments across GPs, specialists, pharmacies, and living rooms, and most of what matters (the emotions, the misconceptions, the workarounds, the reason someone silently stopped a treatment) never makes it into a claims database, an EHR, or a trial record. The patient’s voice is the one input the system was never built to capture.
For decades, the answer was: hire consultants. Commission a market research agency. Wait six months for a 40-page PowerPoint. Repeat. That wasn’t a failure of effort, it was a ceiling on what was feasible. Consultants can only work with the inputs that exist, and what existed was structured, small-sample, and already stale by the time it landed. What mama health is building is a structurally different answer, and it simply wasn’t possible before AI.
This isn’t a data problem. It’s an infrastructure problem. Veeva was an infrastructure problem (CRM built specifically for the life sciences industry that everyone said was too niche). Today it’s worth $30bn. Infrastructure problems, when you solve them properly, tend to produce companies that last.
What they actually built
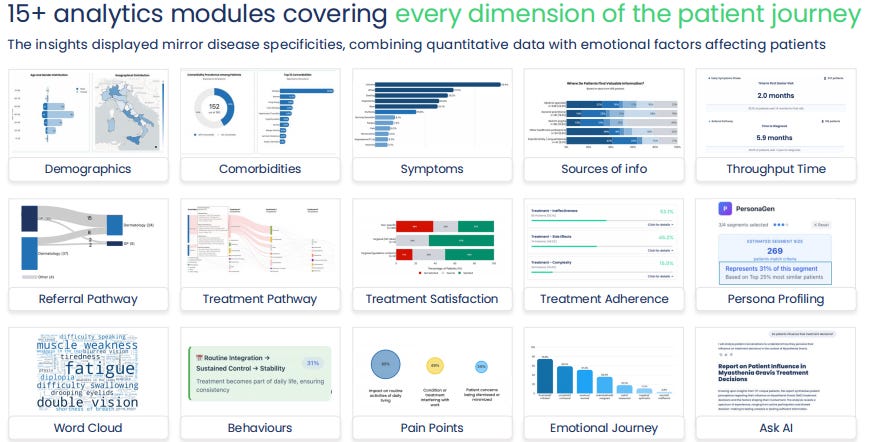
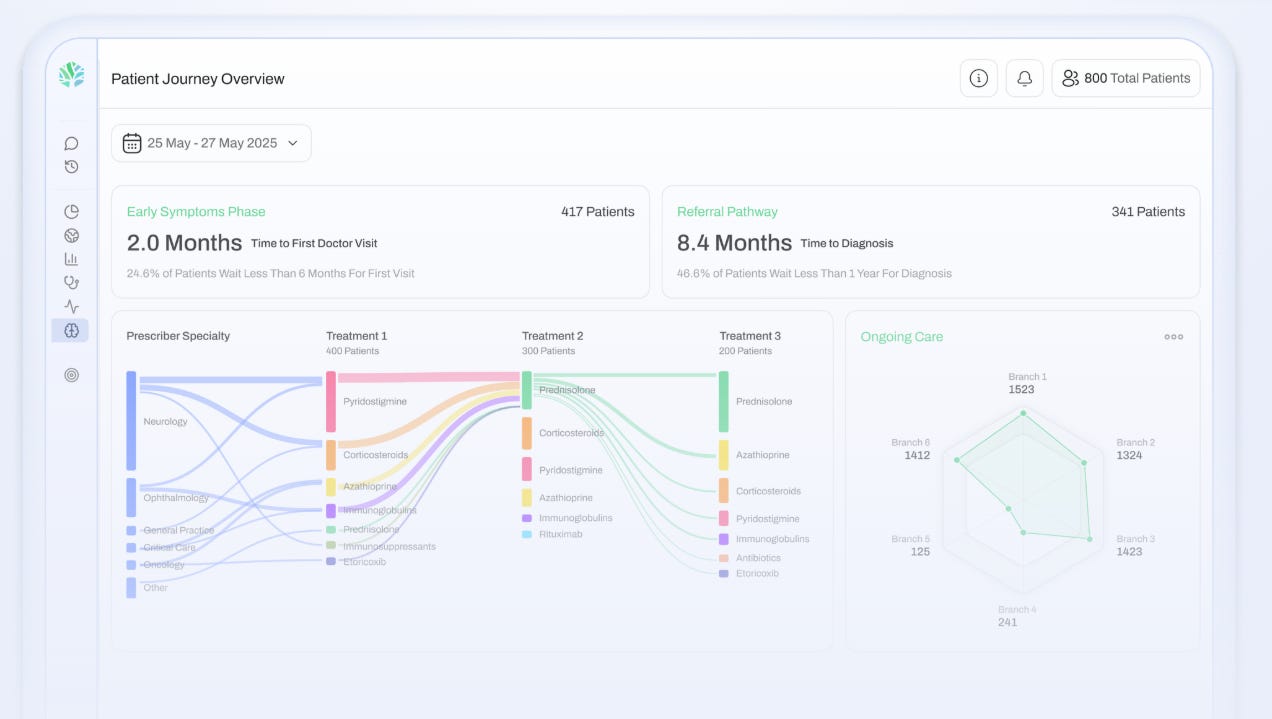
What Mattia and his team built is an AI-native patient intelligence platform, starting from chronic conditions. And the reason chronic conditions matter here is important: if you have diabetes, multiple sclerosis, psoriasis, or myasthenia gravis, you don’t just interact with the healthcare system once. You live with your condition every day. You try treatments that don’t work. You stop taking things without telling your doctor. You find workarounds. You develop fears and misconceptions that never come up in a clinical setting. You have a whole inner life around your disease that nobody ever captures (because nobody ever really asks). That’s exactly what mama health does. An AI companion guides patients through a real conversation about their diagnosis journey, their treatments, their fears, what they wish someone had told them earlier. 150+ data points extracted per patient. Anonymized, structured, fed into a live dashboard that pharma teams can query in real time. Imagine a platform where a brand team, mid-meeting, can ask “why are patients in this indication not reaching specialists?” and get an answer grounded in hundreds of real accounts (I rarely saw customers this excited about a product!).
The reason none of this was possible before is simple. Structured surveys killed the narrative before it started: patients abandoned them, and you couldn’t run enough to matter. If you wanted depth, you needed a human moderator, which meant maybe 20 or 30 interviews before the budget ran out. And even if you somehow collected 500 open-ended conversations, you had no way to turn them into something queryable at speed. LLMs changed both things at once. The mama health team saw that window before almost anyone else.
The doubt I couldn’t (initially) shake
Let’s complicate things.
On paper, mama health is B2B as they sell their “Bloomberg terminal” to pharma. But it only works if the consumer side is active. Which means the product has to be actually useful to a person living with a chronic condition. This is one of the few cases I’ve seen where B2B and B2C don’t just coexist but are structurally dependent on each other. As if scaling a B2B or B2C platform was not complex enough, they decided to do both at the same time. The classic examples of this working are the great marketplace companies: Airbnb needed hosts and guests simultaneously, Doordash needed restaurants and customers. Neither side had value without the other. mama health is the same logic applied to healthcare.
Now here is where I have to be honest. I really believe that in venture, if something feels obvious to everyone, you are probably already too late. We knew there was “something”, and we had initially many questions and doubts (I remember calling Irene probably 10 times per day during the first phase).
We did nearly 20 expert calls in two weeks. We spoke to people at Novartis, AstraZeneca, UCB, pharma consultants, former founders in the space, people who had spent decades on exactly this problem. And the thing that kept coming back (the concern I couldn’t shake for a while) was: selling to pharma is brutal and slow, and you can’t sell across geo. I mean that seriously… Pharma procurement is notoriously difficult. Sales cycles are long, sometimes nine months or more. Every country has its own governance, its own compliance requirements, its own approval chain. The incumbents (think about the IQVIA, the big consultancies) have spent years building the trust and the vendor relationships that let them operate at scale.
One senior reference was blunt about it: getting a new solution past legal, medical affairs, and the central budget holder at a large pharma company is genuinely hard, and most startups that try underestimate what it takes. So the question we kept asking ourself was: are these guys actually breaking through, or are they collecting a few early enthusiast contracts that plateau the moment they try to scale beyond their network?
What answered that question (after we decided to invest!) was watching what happened in real time. In the months between our first call and closing, we watched one customer expand from one country to nearly ten, a 10x increase in ACV from a single account. A customer reference gave them a 10 out of 10 NPS and said she would want it across every therapeutic area she touched.
When I spoke to Luca Foschini, who built Evidation Health and knows this market better than almost anyone, the first thing he said was: “I wish this was around when we were building Evidation.” That’s the thing about pharma. It is brutal and slow to break into. But once you’re in, once you’ve proven value inside a brand team that has real stakes, the expansion is organic and the stickiness is real. People don’t rip out tools that have become part of how they think about a launch.
Why we invested
After months getting to know the founders, nearly 20 expert calls with pharma insiders at Novartis, AstraZeneca, UCB and others, and watching the traction inflect in real time, we decided to invest. Here are the five reasons we said yes, in clearly labelled highlights.
An infrastructure play in a market starving for one
Pharma commercial teams spend over €500M on every single drug launch, and 40% of those launches underperform. The industry still runs on static, consultant-delivered market research that’s outdated the moment it ships. The opportunity isn’t to sell a better research report, but to become the layer every brand team, every medical affairs team, and eventually every payer and regulator uses to understand how patients actually live with disease.
The right product was just made possible
In the last 12–24 months, two binding constraints collapsed simultaneously: (i) the need for a human moderator to get patients to open up, which capped every study at maybe 30 interviews, and (ii) the inability to turn thousands of open-ended conversations into something queryable at speed.
LLMs and multi-agent orchestration dissolved both at once. The result is 10x more patients than standard research, at a fraction of the cost, with the depth traditional research never had.
A founder-operator team built exactly for this problem
Mattia (CEO) spent years on the commercial side of pharma. He knows the language, the decision cycles, the budget owners. He’s the kind of founder who makes you feel slightly behind in a conversation, mostly because he’s clearly thought harder about his market than anyone in the room. Jonas (COO) is a medical doctor with a PhD in Neuroscience, who, convinced of the singularity idea and experiencing first-hand the tsunami of innovation disrupting healthcare, decided to switch sides and become the builder of the future that his colleagues will suddenly see happening. Johannes (CTO) is a rare disease patient and has built his own company before. Lorenzo (Chief AI Officer) has a PhD in AI for Health and 30+ peer-reviewed publications on AI/ML in medicine. Luca (CFO) spent years in investment banking and then in a health tech start-up.
Bonus pic: the CEO bringing croissants on day 1 in the new Berlin office.

Traction that de-risks the thesis
In under two years, mama health has gone from zero to a book of clients that already includes 6 of the 20 largest pharma companies in the world, with a meaningful share of them expanding beyond their first license.
A data moat that compounds with every conversation
The moat is the data: long-form, first-person patient narratives, refreshed daily across a growing set of indications and geographies, which claims, EHRs, consultants won’t be able to provide. The only way to build it is bottom-up, one patient at a time, owning the relationship, earning their trust and giving them a reason to log back.
Where our community can help
If you work in pharma commercial teams (brand, medical affairs, market access, patient advocacy) or have relationships there, especially in chronic, rare, or immunomediated conditions, we would love an introduction.
The one question to ask: does this team have a pre-launch or launch-stage program where understanding the patient journey is a live priority?
Reach out to us directly, or get in touch with Mattia at mama health.
Virgi

